Elbow Problems
Discover Relief for Elbow Problems
At shoulder2wrist, we understand the impact that elbow pain can have on your daily activities. Our team is here to help you find effective solutions for various elbow issues:
Pain: Elbow pain can stem from various conditions, and we are dedicated to identifying the underlying cause and providing targeted treatment.
Stiffness: Whether arising from an injury or related to arthritis, we offer therapies to reduce stiffness and enhance flexibility.
Tendon Injuries: Injuries to the biceps or triceps tendons may occur, and our experts can guide you through the recovery process, including necessary repairs.
Tendon Irritation: Conditions like tennis elbow and golfer's elbow can lead to tendon irritation, and our specialised care can ease discomfort.
Elbow Instability: If you experience instability in your elbow, even without a specific injury, our team can address this issue and provide appropriate support.
Osteoarthritis / Rheumatoid Arthritis: Elbow joint arthritis can be managed effectively through personalised treatment plans.
Fractured Bones: Elbow fractures can be complex, but our skilled team is experienced in handling such cases.
Taking Steps Towards Relief
There are self-care measures you can try to alleviate elbow pain, including painkillers and ice packs to reduce inflammation.
If your symptoms persist or impact your quality of life, consider seeking professional treatments:
Physiotherapy: Tailored exercises and therapies can aid in restoring elbow function and minimising pain.
Injections: Our experts may recommend injections to help manage discomfort effectively.
Surgical Options: In certain cases, surgical intervention may be necessary, and we can guide you through the process with expertise and care.
At shoulder2wrist, our mission is to provide comprehensive care, guiding you towards improved elbow health and a pain-free life. Don't let elbow problems hold you back - take the first step by scheduling a consultation with our experienced team today.
What is tennis elbow?
Tennis elbow (lateral epicondylitis) is typified by pain on the outside of the elbow. The pain is caused by inflammation of the tendons that extend the wrist. It starts with repetitive overloading, which causes small tears in the tendon. When these don’t heal fully, the quality of the tendon reduces and the pain is exacerbated.
Before you come and see a surgeon
If your GP believes you have Tennis elbow, they may arrange an ultrasound scan and an x-ray to confirm the diagnosis prior to referring you for physiotherapy. If required, we recommend ONLY ONE injection of steroid under ultrasound guidance. There is now evidence that multiple injections can cause long-term skin changes and may prevent full recovery even after surgery. In the vast majority of cases, things will settle down by around 6 months to one-year.
Outpatients
Your surgeon will examine your elbow and may perform some tests that cause pain; these are important to confirm the diagnosis. Usually, we will check that you’ve had an x-ray and an ultrasound to confirm the diagnosis but these are not always necessary. In cases of previous failed tennis elbow surgery we will normally arrange an MRI scan.
What is the treatment?
Tennis elbow responds well to the correct physiotherapy regime. In addition, a course of anti-inflammatory medications and a tennis elbow clasp may help. If you have not previously had one, an injection of steroid may be considered. If you fail to respond to the above measures, we may discuss surgery with you.
Tennis elbow release surgery can be done through open or keyhole surgery. In both cases, inflammation and scar tissue is removed from the attachment of the tendon. The benefit of keyhole (arthroscopic) surgery is that the whole joint can be inspected and additional pathology treated at the same time.
After the surgery
The elbow is protected in a bulky bandage that can be removed after one week. The wound should be kept dry, clean and covered until 2 weeks postoperatively. The elbow can be moved gently from Day 1 postop but you should try and avoid activities that cause pain. You can return to normal activities from 6 weeks as pain allows.
Outcome
Surgery is successful in around 90% of cases, but the duration of time it takes to improve is very variable (generally 3-6 months for full resolution). In some cases there remains some mild pain during exercise and very rarely there is no improvement following surgery.
What is Golfer’s elbow?
Golfer’s elbow (medial epicondylitis) is typified by pain on the inside of the elbow, where the flexor muscles of the wrist attach. It usually starts with inflammation as a result of overloading the wrist, followed by microscopic tears in the tendon, which may not heal. The quality of the tendon then deteriorates exacerbating the problem.
Sometimes, the problem is associated with an irritable or compressed ulnar nerve on the inside of the elbow. This may cause tingling and numbness in the ring and little finger, and occasionally a reduction in grip strength.
Before you get referred to a surgeon
If your GP believes you have Golfer’s elbow, they can arrange an ultrasound scan and an x-ray to confirm the diagnosis prior to referring you for physiotherapy. In the vast majority of cases things will settle down by around 6 months to one-year.
Your clinic visit
Your surgeon will take a history of the problem and examine you with some special tests, which may provoke pain. Usually, a minimum of an X-ray and an ultrasound are requested or the results reviewed, but this is not always necessary. If you have problems affecting the nerves around the elbow we will arrange nerve conduction tests to confirm the diagnosis.
What is the treatment?
The best treatment for Golfer’s elbow is physiotherapy, and surgery is only considered in those patients who have undertaken a good course of treatment with the correct regime. Taking anti-inflammatory medications and very occasionally having a single injection can increase the success of the physiotherapy.
Operation
The operation is an open procedure. Inflammation and scar tissue is removed from the attachment of the tendon, which is then repaired back to bone if necessary. The ulnar nerve can be released at the same time or moved if it is considered unstable in its normal groove. For complex or repeat cases the whole muscle group can be lengthened (fractional lengthening) which has equal results to other techniques but may prevent further problems associated with a painful superficial scar.
After the surgery
The elbow will normally be placed in a bulky dressing. This should remain in place for 5 days but the elbow can be moved gently within the confines of the dressing. It can then be removed to reveal a surgical dressing, which should remain and be kept dry until 10 days has passed. If the nerve has been relocated we occasionally place you in a plaster splint for 2 weeks prior to mobilizing the elbow.
Splints and dressings are removed at your first followup appointment or by a GP practice nurse. The elbow can then be moved fully though we ask you not to load it for 6 weeks; straightening the elbow is often difficult at the start. After six weeks, the elbow may be used again as able.
Complications
The general complications include bleeding, infection, pain and stiffness. The serious but rare complications include nerve injury, ligament injury causing elbow instability and chronic scar pain. If you get recurrence of your problem you might require further surgery in the future.
Results
The results of this operation are good or excellent in 95% of patients. The worst outcomes are seen in those patients with significant involvement of the nerve associated with muscle wasting. In a small percentage, there remains some mild pain or discomfort during exercise and in a very small percentage there is little improvement following surgery, or they may feel it’s made them worse.
Most patients will regain mobility of the elbow by around 2-4 weeks and start to feel improvement from 6 weeks onwards.
Distal Biceps Rupture
The biceps muscle is on the front side of the upper arm and gives the arm its characteristic shape. The tendon travels across the front of the elbow and attaches to the top of the radius bone. The biceps primarily functions to turn the palm of the hand upward (supination) but also bends the elbow. The tendon usually tears because of sudden excessive loading.
Most patients are men associated with heavy lifting. Occasionally the patient reports a longer-term problem affecting the arm, which might indicate a more inflammatory, scarred process.
In Outpatients’ Clinic Your surgeon will arrange an x-ray and examine your arm. There may be bruising and a deformed contracted biceps muscle. When asked to use the muscle it may be painful. The doctor will try to feel the tendon and compare it to the other side. The tear may be partial or complete and if there’s any doubt an ultrasound or MRI scan (FAB view = a special position of the arm) is normally arranged.
It is vital that you are clear about when the injury or rupture occurred. The longer you leave it the more difficult the surgery and the increased risk of significant and limb threatening nerve or vessel damage during surgery. We will not normally offer repair beyond 4 weeks and ideally prefer to perform the surgery in the first week following the injury.
What is the treatment without surgery?
You do not need to have the tendon repaired. If you choose not to you will have permanent deformity of the arm with a small contracted biceps. Your elbow flexion/bending strength will usually return to near normal as other muscles can take over. Your ability/strength to turn the palm upward (like using a screw-driver) will be significantly reduced. If you have a partial tear in the tendon, this may recover but sometimes reattaching the tendon is required.
What is the treatment with surgery?
For partial tears, the tendon can be visualised and if less than 50% torn can be reattached with an anchor. If greater than 50%, we complete the tear and repair it fully into the bone. The surgery involves freshening the tendon to healthy tissue and then reinserting it into a tunnel, which we create in the bone where the previous tendon insertion was.
After the surgery
The elbow is placed into a bulky bandage dressing and a sling applied. Very occasionally, a plaster is used for a couple of weeks to protect the repair. You can gently move the elbow from the outset if instructed to do so by your surgeon. DO NOT load the arm for 6 weeks and return to heavy lifting should be delayed for at least three months if not longer.
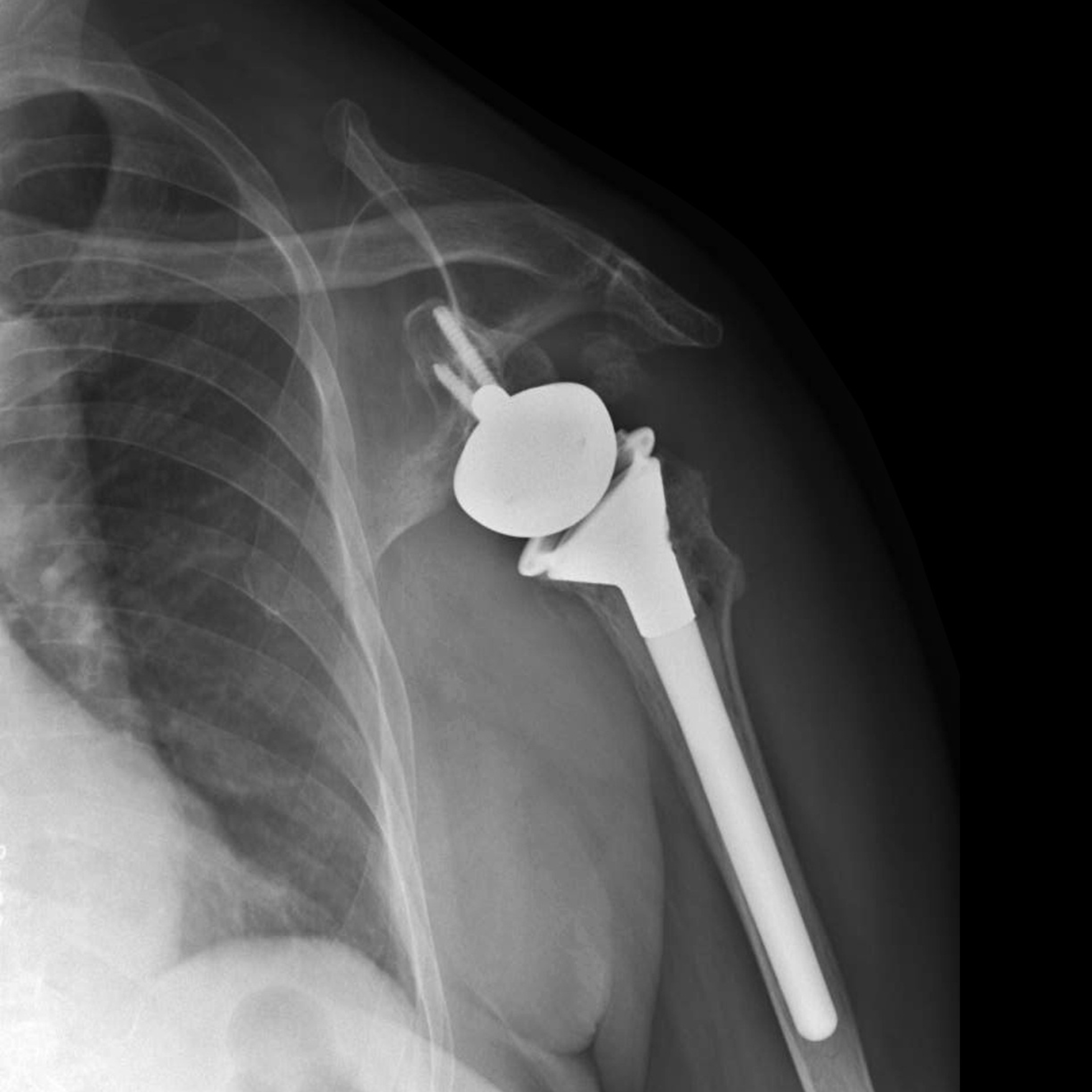
Introduction
Total elbow replacement is carried out when the elbow is no longer functioning properly. This may be for a variety of reasons – inflammatory arthritis, complex fractures, tumour or osteoarthritis.
The Operation
The procedure is done under general anesthesia (asleep) in addition to a nerve block for pain relief. You are positioned on your side and a tourniquet is placed around the top of the arm to prevent bleeding during the surgery. The incision/cut is made on the back of the elbow and once the new elbow has been cemented in place, the skin is closed. A bulky bandage and a simple sling is applied to enable gentle but early range of movement.
After surgery
Unless instructed otherwise, you can bend your elbow to bring your hand closer to your mouth and let gravity straighten your elbow. YOU MUST NOT push up out of a chair or shove anything using your arm for 6 weeks. For the rest of your life you should not be lifting objects heavier than 1.5kg for repetitive tasks. When lifting weights, damage to your elbow can be prevented by keeping the elbow alongside your body.
Complications
The main complications are infection and wound problems. If this occurs and is caught early, the prosthesis can be saved by further surgery to wash the elbow out and antibiotics through a drip. If an infection is caught late, it is usually necessary to remove the elbow replacement to eradicate the infection before a new replacement can be implanted. Nerve injury is very rare and most commonly injured temporarily. Permanent nerve injury is more common in revision surgery or following infection.
Results
Elbow replacements results are very varied. 90% will work well for a period of around 10 years; some will last 5 and others 20! Loosening of the prosthesis is the most common long-term problem and this can cause fracture of the bones around the elbow. In these cases a more complex revision to implant a new elbow replacement may be needed.
Introduction
The elbow is commonly injured following a fall on to the outstretched arm. These type of injuries affect all ages from children through to the very elderly. No matter what the injury, the key to a successful outcome is to mobilise the elbow early to prevent stiffness. If the elbow is unstable, then surgery must be undertaken to stabilise the elbow to allow early range of movement.
Elbow fractures
The elbow is made up of three bones and three joints. The humerus, ulna and radius move in a particular way to produce bending and straightening the elbow, and turning movement to place the palm of the hand face up and down. There are many different fractures around the elbow. Most can be managed without surgery but some injuries require surgery to ensure a satisfactory outcome.
Elbow dislocation
Elbow dislocation is very common and the vast majority do not require any surgical intervention; these are dislocations without an associated fracture (so-called “simple” dislocations). In “complex” dislocations or those with an associated fracture, surgery is more commonly undertaken to stabilise the elbow to allow early range of movement.
Elbow injuries
A number of patients do not present with a dislocation or an obvious fracture but still clearly have a problem with the elbow after an injury. Occasionally further imaging tests are requested to confirm the diagnosis.
Patient Specific Elbow Deformity Correction….. Materialise